
(Art design: Jean-Dominique Lavoix-Carli)
As the global fifth wave of the COVID-19 pandemic has now started, should we be worried about it? How lethal will it be?
This article and the next will focus on direct health-related impacts of the COVID-19 pandemic fifth wave. Indeed, these effects are those that determine all others. Here, we shall look at the potential lethality of the fifth wave. The next article will address the Long-Covid, a key yet rarely accounted for aspect of the pandemic.
We focus, first, here, on the lethality of the previous waves and examine if a pattern emerges. Then we address the various factors that will impact the lethality of the fifth wave, notably the two anti-viral treatments of Merck and Pfizer and the waning vaccinal immunity after six months. We use the U.S. as case study and, adding the case of Israel, we deduce possible global trends. We also highlights some hurdles that political authorities could face regarding the acceptance of the 3rd dose.
This series on impacts of the COVID-19 fifth wave is the second part of the previous article: “Towards a Covid-19 Fifth Wave?“. There, we assessed it was very likely the global start of the fifth wave of the COVID-19 pandemic had taken place at the end of October 2021. There we also highlighted the factors that would shape this fifth wave. We now use the elements identified in this first article as basis to ground our evaluation of impacts.
Global deadly waves of Covid-19
Using the available global statistics, unsurprisingly, we find a periodicity of waves of death similar to what we found with infections.

The deadly impact of the waves of contagion
Deadly impact in two phases for the first global contamination rise – until 17 October 2020
The first wave – the global contamination rise – lasted from December 2019 to 9 October 2020. It corresponds to a wave of deaths that lasted until 17 October 2020, i.e. 8 days after the turn towards the second wave of contamination.
However, here we have distinctively two phases. The first phase peaks around 15 April 2020 with 8.905 death per day, then recedes to 4.677 deaths on 26 May 2020 and 3.628 on 1st June. This is the lowest global number of death since the start of the pandemic. By 3 November 2021 (8.078 deaths), we have so far not yet lowered again the level of daily deaths to this number.
As far as the very early stage of the pandemic is concerned, the high number of death compared with the low number of infection shows the global unpreparedness as well as lack of medical understanding, then, of what was a completely new illness.
The second phase of this first wave is a slowly ascending plateau from 4.677 to 6.056 deaths per day, with small peaks, showing the global spread of the illness, while medical knowledge nonetheless improved.

As a whole 1,16 million people lost their lives during this first wave (figures from “Cumulative confirmed COVID-19 cases and deaths, World“, Our World in Data).
For the sake of comparison, a 2019 study estimates the global number of deaths from influenza amounts to 400.000 per year, i.e. almost three times less (Paget, John et al. “Global mortality associated with seasonal influenza epidemics: New burden estimates and predictors from the GLaMOR Project” Journal of global health vol. 9,2, 2019, doi:10.7189/jogh.09.020421).
From the second to the fourth wave
The second wave
The deadly second wave lasted from 17 October 2020 until 9 March 2021, with a low at 10.524 deaths per day. The shape follows closely the shape of the wave of contamination with a first peak on 22 December 2020 at 15.430 deaths per day followed by a higher peak on 27 January at 18.357 deaths per day. It lasted around four months and three weeks.
The second wave represents 1,54 million deaths.
Compared with the second wave of contamination, the deadly wave started one week later, the peak of daily deaths took place 13 days after the contagion peak, and the end of the wave took place 20 days after the end of the wave of infections.
The third wave
The third wave, in terms of daily deaths thus started from around 10 March 2021 and lasted until 28 June reaching then 6.909 deaths, i.e. 65% of the previous low. The peak happened around 28 April with 15.471 deaths, i.e. 84% of the previous peak. The wave lasted thus approximately 3 months and two weeks.
Compared with the infections, the deadly wave started 3 weeks later, the peak occurred surprisingly one day before the peak of contagions. The deadly wave ended one week after the wave of infections.

The third wave represents 1,23 million deaths. Actually, it is likely this figure is vastly underestimated. Indeed, the third wave includes the tragic spread of the Delta variant in India. A study using three different types of methodologies concluded that the death toll for India only between the start of the pandemic and June 2021 could be between 3.4 million and 4.9 million excess deaths (Abhishek Anand , Justin Sandefur and Arvind Subramanian, “Three New Estimates of India’s All-Cause Excess Mortality during the COVID-19 Pandemic“, Center for Global Development, 20 July 2021. These figures must be compared with the official death toll that counts 339.053 death on 1st June and 399.459 on 30 June 2021 (e.g. Financial Times).
The fourth wave
The fourth deadly wave started around 28 June 2021, lasting until 17 October 2021 with 4.067 daily deaths, i.e. 59% of the previous low. The peak occurred around 26 August 11.717 deaths, i.e. 75% of the previous peak. The wave lasted around 3 months and slightly less than 3 weeks.
Compared with the infections, the deadly wave started 1 week later, the peak occurred also one week after the peak of contagions. It ended on the same day as the wave of infections. In other words, the fifth wave started surprisingly being felt in terms of deaths without any time lag. This likely comes from the various stages of waves for individual countries mixed with varying vaccination and induced-immunity. This shows the limits of relying uniquely on global aggregated data when we need to evaluate the potential lethality of a wave.

The fourth wave represents 0,97 million deaths.
To understand better what this means in reality, let us give a couple of comparisons.
For the U.S., during the fourth wave, 131.276 (732.634 – 601.358) Americans died of COVID-19. This is 2,46 times more than the Americans who died fighting during World War I (53.402), almost half (45%) of those who died during World War II (291,557), 3,88 times more than those who died fighting during the Korean War (33,686), 2,76 times more than those who died fighting during the Vietnam War (47,434) (Wikipedia, United States military casualties of war). And this is for the least lethal of the last three waves of COVID-19.

Of course, the relative importance of wars compared with the pandemic waves will vary according to countries. However, considering the influence of the U.S. in the world as a superpower, it is key to understand that the COVID-19 so far as been more deadly for the U.S. than any other war it waged in the world.
The COVID-19 has killed more Americans than World War II that counted 405.399 American deaths (all causes of death – Wikipedia, ibid.). The pandemic has even been more deadly than the Civil War (1861–1865), the most lethal conflict the U.S. has ever known so far. Then, the number of deaths is estimated to 655.000, while by 7 November 2021, the COVID-19 pandemic has killed 752.196 Americans (CDC data, 7 November 2021).
A pattern for the lethality of the waves?
What can we deduce from the lethality of the four first waves of COVID-19? Is there a pattern and an evolution emerging that may help us evaluating lethality for the future and more specifically the fifth wave?
As far as lethality is concerned, the periodicity and length of the waves are far less regular than those of infections. Similarly, the relationship between, on the one hand, the wave of infections, and, on the other, its impact, the number of deceased, is also irregular.
- Niger: a New Severe Threat for the Future of France’s Nuclear Energy?
- Revisiting Uranium Supply Security (1)
- The Future of Uranium Demand – China’s Surge
- Uranium and the Renewal of Nuclear Energy
- AI at War (1) – Ukraine
- Anticipate and Get Ready for the Future – Podcast
- The Return of Nuclear Energy
- Climate Change, Planetary Boundaries and Geopolitical Stakes
The main reasons for the differences and irregularities lie probably in the very diverse capabilities of health systems according to countries, added to the heterogeneous availability type, and spread of pharmaceutical treatments and vaccines.
If we do not consider the very likely reality of the third wave in India compared with official estimates – which is a very big if – then, since the second wave, we see an overall diminution of the lethality of the waves of COVID-19.
The global trend for the last three waves would tend to indicate a diminution of the height of the waves – the peaks of daily deaths are successively lower for each wave, while the lower points are also similarly lower. Again, the reasons for this overall diminution of deaths are most probably a mix between an improvement of medical treatment and capabilities of health systems to handle the illness, alongside the spread of vaccination.
Thus, looking at this general trend, we could start our assessment with, as baseline, a wave lasting until the end of the wave of infections, i.e. around 20 February 2022 and peaking between 20 December 2021 and 20 January 2022. If the favorable trends towards less lethal waves of the pandemic continues, we could have a peak around 50% of the previous one, i.e. 5.858 deaths, and a low around 50% of the previous wave. i.e. 2.034 deaths.
However, the reality of the impact of the Delta variant in India cannot be ignored. This strongly stresses that our collective global efforts must be directed at preventing variants of concerns (VoC) to emerge and spread. They are indeed a major factor of lethality.
Our total inability to anticipate the emergence of new VoC, apart knowing that the more the virus circulate, the more likely a VoC will emerge makes it difficult to assess in advance the lethality of a wave. However, as we saw, borders’ control throughout the world, and notably in the U.S. are being relaxed (see Towards a Covid-19 Fifth Wave?; Reuters, “What you need to know about the new U.S. international air travel rules“, 7 November 2021). This considerably heightens the likelihood to see a VoC emerging and spreading, hopefully not for the fifth wave.
Besides VoC, assuming health systems capabilities and medical practice remain constant the availability of new treatments, vaccination and the length of induced immunity are the factors most likely to influence the lethality of the wave, as we shall now see.
Factors impacting the lethality of the COVID-19 pandemic waves
Too early or or just in time for the new anti-viral treatments?
In October and November 2021, two new antiviral treatment, easy to administer came to the fore. What are these treatments? Are they the anti-COVID-19 treatments that will allow us finally overcoming the pandemic?
Monulpiravir (Lavgevrio in Britain)
U.S.-based Merck & Co Inc and Ridgeback Biotherapeutics developed the new antiviral pill using the molecule molnupiravir. It has been authorised in the UK on 4 November 2021 under the name Lavgevrio and could have a positive impact on lethality (Pushkala Aripaka, “Britain approves Merck’s COVID-19 pill in world first“, Reuters, 5 November 2021).
As explained in the video below, Merck’s pills aims “to introduce errors into the genetic code of the virus” and thus generates random mutations (Deena Beasley, “Explainer: How does Merck’s COVID-19 pill compare to Pfizer’s?“, Reuters, 8 November 2021). It is also believed that, as a result, variants of concern will not evolve, as the mutations are random (ibid.).
At the probable start of the fifth wave of COVID-19, we only have the results of the phase III trial of the company, stemming from “a planned interim analysis [that] evaluated data from 775 patients” (Merck, News Release 1 October 2021). According to the company, if “at risk, non-hospitalized adult patients with mild-to-moderate COVID-19″ receive twice a day four pills for five days within five days of the onset of symptoms, then “molnupiravir reduced the risk of hospitalization or death by approximately 50%” (Ibid.; Aripaka, “Britain approves Merck’s COVID-19 pill in world first“, Reuters, 5 November 2021; Deena Beasley, “Explainer: How does Merck’s COVID-19 pill compare to Pfizer’s?“, Reuters, 8 November 2021).
The very interesting video by Dr. Seheult of Medcram helps understanding better the new treatment, how it works and the trials.
For readers who are not fluent in English, use translated captions:
Click on the small wheel (“Settings”) just before Youtube on the bottom right hand side of the video player.
Click on “subtitles”, then on “auto-translate” and then choose your language.
Furthermore, the way Great Britain will use the pills is still experimental (Aripaka, ibid.). Finally, safety data for the drug are not public for now (Aripaka, ibid.).
Pfizer’s Paxlovid
Pfizer’s drug is not yet authorised on 8 November 2021 and was annouced by the company on 5 November 2021 (Pfizer, News Release). It will be commercialised under the name Paxlovid (Ibid.).
The active molecule, used in combination with an older antiviral ritonavir, is “part of a class known as protease inhibitors designed to block an enzyme that the coronavirus needs to multiply. Pfizer said that because the drug targets a part of the virus essential to replication, the pathogen cannot become resistant to the treatment” (Beasley, “Explainer“, Ibid.).
Pfizer phase 2/3 trial for the “Evaluation of Protease Inhibition for COVID-19 in High-Risk Patients” began enrollment in July 2021, and two other studies, one for Standard-Risk Patients and one for Post-Exposure Prophylaxis are still ongoing (Pfizer, News Release, 5 November 2021). “The primary analysis of the interim data set evaluated data from 1219 adults who were enrolled by September 29, 2021” (Ibid.). Safety evaluation used a larger cohort of 1881 patients and continues (Ibid.).
According to Pfizer, for high risk patients, the drug was found to reduce the risk of hospitalisation or death by 89% if given within three days of symptom onset and by 85% if given within five days (Ibid.). Pfizer’s regimen is three pills in the morning and three pills at night (Beasley, “Explainer“, Ibid.).
Too early for a global impact on the fifth wave?
Results for Pfizer’s drug are thus much better than for Merck’s pills, and because they involve less pills might be more easily available. However, as for Merck, there are no independent studies, the number of patients who have used the pills is small and the trials are so recent that secondary effects, especially on medium and long term, can hardly be known with certainty.
It is thus too early to consider widespread and global use of the pills and impact. Furthermore, to envision such a global impact we would also need to take into account manufacturing.
What happens in the UK regarding the use of Molnupiravir will need to be closely monitored.
But panic leads political authorities to discard precautionary principles
Nonetheless, we should also note that countries, for example Indonesia as well as “The United States, Malaysia, South Korea, Singapore, Thailand and the Philippines”, are hurrying up to authorise and pre-order Merck’s treatments, and most probably Pfizer’s (Reuters, “Indonesia reviewing Merck COVID-19 pill, up to 1 mln doses targeted“, 8 November 2021; Merck, News Release 1 October 2021; Pfizer’s news. Ibid.). They may thus have impacts – positive and negative – earlier than caution and safety would require.
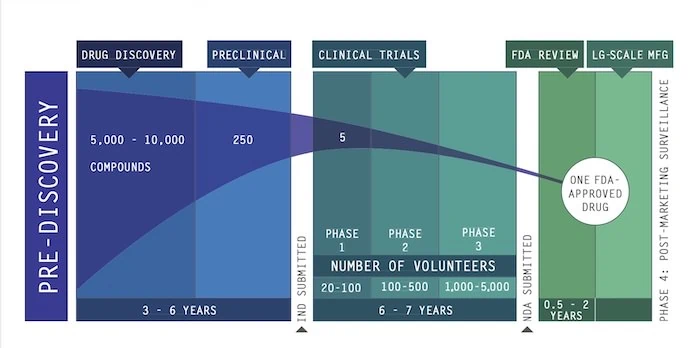
It is worth here highlighting again that, usually, discovering a new drug and especially testing it takes a much longer time than what was done in the two cases of the antiviral pills, for example the 3 months of phase 2/3 trial for Pfizer, as we stressed in our earlier article “COVID-19 Antiviral Treatments and Scenarios“:
Once it is discovered, the new potential drug will have to go through the whole process of trial and development, including clinical trials (e.g. EU Drug Discovery and Development, U.S. Biopharmaceutical Research & Development).
Classically – i.e. when we are not in an emergency mode – this process takes 10 to 15 years (Drug discovery, Ibid.) as shown in the picture below:
Helene Lavoix, “COVID-19 Antiviral Treatments and Scenarios“, The Red Team Analysis Society, 30 March 2020.
Here phases for clinical trials have been extraordinarily reduced. If things go well, then it will be perfect and optimism will triumph. If not, then we may be facing a tragic disaster, or even multiple disasters. The rule in strategic foresight and early warning is to always consider high impact scenarios even if the scenario is unlikely, for example when building wild cards scenarios (see Course on scenarios). This is what ought to be done.
Meanwhile, manufacturing of the pills has only started. However, Merck asserts that it could have manufactured 10 million courses of its treatment by the end of 2021 and more for 2022, at least 20 million according to Beasley for Reuters (Merck, News Release 1 October 2021; Beasley, “Explainer“, Ibid.). For its part, Pfizer would have 180.000 courses ready by the end of 2021, and 50 millon by the end of 2022 (Beasley, “Explainer“, Ibid.). Thus should these announcements all be correct and no bad surprise emerge, then severe illnesses and deaths could be significantly reduced (at least by 50%) for countries taking these drugs, before the end of the fifth wave.
We should consider widespread usage of these pills initially as an outlier that must be closely monitored.
For now, for the fifth wave, vaccination remains the major factor to consider as potentially altering the lethality of the fifth wave.
Vaccination, Immunity and lethality
If we want to have a better assessment of the lethality of the fifth wave of COVID-19 we need to consider vaccination.
Safety of the third dose
Note that we shall assume below that there are no serious side effects and safety concerns on the medium to long term for the third dose of vaccination. The existence or absence of such safety concerns is so far unknown. Israel, the first country to do so, authorised the administration of the so called “booster shot” on 30 July 2021 (Yinon M. Bar-On, “Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel“, October 7, 2021, N Engl J Med, 2021; 385:1393-1400, DOI: 10.1056/NEJMoa2114255). It is thus too early to know if there are any negative effects on the medium to long-term.
On the short term, according to the ongoing monitoring of the U.S. CDC (the US started administering booster shots on 12 August 2021), most effects reported were similar to those of the first doses (“Fever, headache, fatigue and pain at the injection site were the most commonly reported side effects”). They are estimated as “mild to moderate” (for 92% to 94% of reports). Nonetheless, 6% of reports were tagged as “serious” (“reactions reported after getting a booster shot”, on data “from August 12–October 10, 2021 for persons aged 12 years and older”).
When vaccinal immunity wanes
For our purpose, most aggregated statistics available are difficult to use. Indeed, these statistics were created for the initial “race to vaccination”, which took place during the first semester of 2021. They thus tend to show mainly the percentage of a population that has received one dose or two doses of vaccines, sometimes using the more relevant criteria of full vaccination scheme. Then they compare countries.
However, what matters to us is not only the proportion of a population that benefits from a full vaccination scheme, and how advanced or late a country is compared to others, but also when vaccination took place and for which proportion of the population.
Let us explain further why this matters.
Vaccinal immunity wanes “considerably” six months after the full vaccinal scheme
As we saw in the previous article, as the case of Israel shows, and as most governments now admit when they emphasise the need for a third dose, the immunity induced by many vaccines against the COVID-19 wanes. This waning certainly takes place after six months, and even possibly before according to vaccines (e.g. US CDC “Infections in fully vaccinated persons: clinical implications and transmission” in Science Brief: COVID-19 Vaccines and Vaccination – update 15 September 2021; Matthew Loh and Hilary Brueck, “Pfizer’s COVID-19 protection against infection may wane in months, but it still prevents hospitalization and death for at least 6, new studies suggest“, Insider, 8 October 2021).
This is also true for the Chinese vaccine CoronaVac from Sinovac, as scientists have shown that immunity falls after six months. A Chinese study concluded:
“Our study found that a two-dose vaccination schedule of CoronaVac (3 μg formulation) generated good immune memory. Although the neutralizing antibody titer dropped to low levels 6 months after the second dose, a third dose was highly effective at recalling a SARS-CoV-2-specific immune response, leading to a significant rebound in antibody levels.”
Hongxing Pan et al. “Immunogenicity and safety of a third dose, and immune persistence of CoronaVac vaccine in healthy adults aged 18-59 years: interim results from a double-blind, randomized, placebo-controlled phase 2 clinical trial“, medRxiv, 25 July 2021.”
Considering that such a large proportion of the world population uses the Chinese CoronaVac, which is administered in 26 countries and part of the global COVAX scheme, the results of Hongxing Pan et al. are key in terms of the global lethality of the fifth wave, as well as, potentially for next ones.
Update 25 November 2021: According to studies from Israel, a third dose administered at 5 months is highly effective in increasing protection against hospitalisation, severe forms of COVID 19, and death compared with two doses at least five months before. For example:
“Vaccine effectiveness evaluated at least 7 days after receipt of the third dose, compared with receiving only two doses at least 5 months ago, was estimated to be 93% (231 events for two doses vs 29 events for three doses; 95% CI 88–97) for admission to hospital, 92% (157 vs 17 events; 82–97) for severe disease, and 81% (44 vs seven events; 59–97) for COVID-19-related death.”
Noam Barda, MD et al., “Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: an observational study“, The Lancet,
Published:October 29, 2021, DOI:https://doi.org/10.1016/S0140-6736(21)02249-2
It would have been interesting to have similar studies checking more precisely when the full scheme of vaccination had taken place (5 months ago, 6 months ago, 7 months ago for example) to have a better understanding of the immunity boost on the one hand, waning on the other. Calculations below are don on the 6 months timeframe for an imperatively needed booster injection and not five months. If ever the truly dangerous waning generalised at 5 months, then results below must be adapted accordingly, The burden and risks are increased.
Waning immunity after six months and impact on the lethality of a wave
Thus, to estimate the lethality of the fifth wave, we must consider that at approximately 180 days after full vaccination, because levels of antibody will have strongly declined, the severity and lethality of the COVID-19 tends towards levels “similar” to those that would be known without vaccination. We do not know how fast a return to full lethality of the COVID-19 will take place. We do not know the proportion of the population who will be at risk and when. Both are nonetheless significant enough, considering studies and what happened in Israel (see previous article).
However, when a third dose is administered, enhanced protection against severity and lethality of the COVID-19 returns, for an unknown length of time. We shall only know if the length of immunisation after the third dose is superior to six months, earliest end of January to mid-February 2022, as third doses have started being administered in Israel on 30 July 2021 et in the U.S. on 12 August 2021 (Ibid,, CDC note 2), assuming no other variant of concern spreads.
We had warned about the key uncertainty relative to the length of immunity and the impacts on the idea of herd immunity as well as on the need for follow up vaccines in our article “COVID-19 Vaccinations, Hope or Mirage?” in October 2020. Knowing that if there is critical uncertainty, then we need to monitor the evolution of the key factors, as well as, preferably, to create scenarios, political and health authorities should not be surprised by the reality of the current situation. If an actor is surprised, then it means this actor should urgently revise its system of early warning (see our related training and online courses).
Waning vaccinal immunity, which impact on the lethality of a wave? The case of the U.S.
We now know that there will be an impact, that it will happen after six months and that it should have been monitored. However, how large or small could this impact be?
We are in the realm of trends because we do not know exactly how these dynamics work.
The figures of the Financial Times we use here, as they provide the multi-country historical series we need, consider all vaccination irrespective of age. As less than 18 years old are increasingly included in vaccination statistics, but as these specific vaccinations vary according to country and dates, distortions may be introduced when trying to assess lethality.
We are thus here rather in the domain of crude estimates. Further detailed research at country level would be need. It is nonetheless interesting to detail what could be happening.
For example, the U.S. has vaccinated between 8,6% of its population on 5 March 2021 and 40.6 % on 1 June (Data Financial Times – all ages). Thus, using the 180 days/six months interval, this means that on 5 September 2021 8,6% of its population needed a third dose or risked severe illness and death. By 1st December 2021, it is 40.6% of the population, whatever the age, that will need to have received a third dose.
Let us continue with the U.S. The country started administering the 3rd dose on 13 August 2021. On 4 November 2021, 11.9% of fully vaccinated Americans above 18 years old (11.1% of the total vaccinated population) had received their third dose (CDC statistics). If the 6 months limit for immunity is correct, we should look at the number of people vaccinated six months before 4 November 21, i.e. 4 May, to have an idea of the gap between those who have received their 3rd dose and those who should have received it. This gap represents the people who are facing increased risks of serious illness and death, if they become infected by the SARS-CoV-2. On 4 May 2021 31.7% of the Americans were fully vaccinated. Hence, on 4 November 2021, using total figures, 20,6% (31,7 – 11,1) of Americans are facing again rapidly rising risks of severe COVID or death. Actually this statement should be revised per categories of population (age, comorbidity etc.).
Thus, on 4 November 2021, the total number of Americans truly protected by vaccination is only 37,6% (58, 2 – 31, 7 + 11,1).
This happens when the country opens up its borders notably to air travels (see Towards a Covid-19 Fifth Wave?; Reuters, “What you need to know about the new U.S. international air travel rules“, 7 November 2021).
Note that if we use the proportion of Americans over 18 years old for the current level of vaccination and of booster doses, we obtain a larger coverage of 50,1% (69,9 – 31,7 + 11,9). This figure is however probably incorrect as the historical number for May given by the FT concerns the total of people vaccinated, irrespective of ages.
The U.S. thus starts the fifth wave with 30,1% of its population over 18 years old not vaccinated at all and 20,6% of the total U.S. vaccinated population facing renewed risks. The latter, furthermore, may be lulled into a sense of false security. By 1st December, as seen, it will be 40,6% of vaccinated people that will need a booster dose, knowing that on 4 November only 11,1% had received one. Thus 29,5% will need a booster dose. These figures will evolve with time as more people get a 3rd dose. We are nonetheless far from any herd immunity.
Now, let us look at what happened in the U.S. during the fourth wave (20 June to 20 October 2021). The fourth wave started apparently with 44,7% people vaccinated and ended with 56,4% vaccinated. We could thus think there is an improvement. However, we must consider the vaccinated people who were seeing their vaccine-induced immunity waning as the fourth wave progressed. These people who started being at risk again were those who had been fully vaccinated between 20 January (n.d.; less than 8,6%) and 20 April (25,8%) minus those who had received a booster dose.
The Americans really protected during the fourth wave decreased from 44,7% (minus an unknown number) on 20 June to 44% (52,5 – 8,5% on 5 March) plus those having received their booster dose on 5 September, to 30,6 % (56,4 – 25,8) plus those having received their booster dose 20 October (in the framework of an open-access article it is not possible to give more precise figures).
As a result, during the fourth wave, 131.276 (732.634 – 601.358) Americans died of COVID-19.
Let us assume that this corresponds to an average protection of 45%. If we imagine that the U.S will both slightly increase its vaccination of the population and accelerate its booster dose, we could take an average protection of 50% for the fifth wave, then we would have 119.341 deaths. The more third doses will be given and the more unvaccinated people will be fully vaccinated, the lower the actual figure will be.
However, we can use this type of crude estimate only if infections do not rise. Considering the opening up of borders and travels (ibid.), the decrease of non-pharmaceutical intervention, and possibly the feeling that the pandemic has ended, it is possible not to say very likely that the death toll worsen.
Vaccination and waning immunity, should we be worried about the global lethality of the fifth wave?
It appears clearly from the example of the U.S. that it would be meaningless to try to give a figure for the lethality of the global wave without entering into long simulations. We can nonetheless assess if we should be worried or not.
If we look again at Israel, between 20 June and 25 October 2021, cumulative deaths went from 6.427 to 8.049, i.e. 1.622 people died during the fourth wave. Comparatively, during the previous wave (21 November 20 – 21 April 20), 3.550 people died (6.346 – 2.796 – Our World in Data). Thus, vaccination with waning immunity, but with some non-pharmaceutical measures such as the mask being rapidly reinstated and with borders remaining closed led to a wave that was less lethal than previously by 54%.
From the Israeli and U.S. cases, we can deduce that even if we are very optimistic, we should nonetheless be worried about the fifth wave.
Israel, a country with a high level of vaccination, a highly efficient medical system, a very reactive policy in terms of non pharmaceutical intervention, and a small population succeeded to only halve the deaths caused by the virus as the fourth wave hit it.
The U.S., for its part, is dedicated to vaccination, but has the highest number of deaths in the world caused by the pandemic including because of politically biased relationships to caution. Its perspective for the fifth wave are that many Americans will still die, probably more than 100.000, especially if borders are opened without caution.
Now considering that the rate of vaccination worldwide is still very low (2,994 bn on 4 November 21, i.e. 37,89%), out of which an unknown number is already susceptible to become severely ill again and die, the prospects cannot be very good. We should brace to face again a wave with a high lethality (compared with no pandemic), including because of the reopening of borders.
Globally, in terms of vaccination an immense effort must still be made to fully vaccinate more than 60% of the world population. Yet, vaccination for the 3rd dose must, at the same time, be implemented for people already fully vaccinated, and that as soon as we reach 6 months after the last injection. The effort thus remains immense.
The initial assessment made out of the 2d, 3rd and 4th wave was probably too optimistic, including because, for the first waves, borders were closed. This is not the direction that still prevails at the dawn of the fifth wave.
One more hurdle
For countries which have already implemented a vaccination policy, a supplementary hurdle may exist, that could heighten lethality.
If governments have enticed their citizens in being vaccinated by promising the end of the pandemic and a return to a pre-pandemic time, then these citizens may develop various adverse reactions.
They may not believe a third dose is truly necessary, considering the bias called “belief perseverance” or “persistence of discredited evidence” (see course on mitigating biases or on analytical modeling). They may thus fall prey to conspiracy theories. They may also fail to adopt an appropriate behaviour to protect themselves and others.
If citizens realise that knowledge of the weakening immunity after 6 months was easily available or could have been anticipated, when they were given a contrary message, then they may think that their government is either incompetent or a liar. In both cases, this is very bad news for legitimacy and the capability of said government to implement any policy, including a mass vaccination campaign for the third dose, or any other campaign for non-pharmaceutical intervention.
Thus, according to countries and to the type of policies used for the campaign of vaccination for the first two doses, the fifth wave may become more or less lethal.
Conclusion
In general and globally, lethality, despite efforts, is very likely to continue until vaccination delivers an immunity that lasts and prevents also infections. We should be even more concerned considering the remaining high risks of emergence of new variants of concern, as seen.
The new treatments may completely alter these prospects. However, the risks entailed in spreading these treatments widely is also very high, even if they may materialise only much later.
As a result, the less borders will be opened without considering the 180 days of immunity, the more non-pharmaceutical interventions, notably face masks and quarantines, will be operative and reinstated flexibly, the less lethal the fifth wave will be.